what is the correct pathway for sperm from spermatogenesis to ejaculation
Learning Objectives
By the stop of this section, you will be able to:
- Describe the structure and function of the organs of the male person reproductive system
- Depict the structure and part of the sperm prison cell
- Explain the events during spermatogenesis that produce haploid sperm from diploid cells
- Identify the importance of testosterone in male reproductive part
Unique for its function in human reproduction, a gamete is a specialized sexual practice cell carrying 23 chromosomes—one half the number in trunk cells. At fertilization, the chromosomes in one male gamete, called a sperm (or spermatozoon), combine with the chromosomes in 1 female gamete, chosen an oocyte. The role of the male reproductive arrangement is to produce sperm and transfer them to the female reproductive tract. The paired testes are a crucial component in this process, equally they produce both sperm and androgens, the hormones that support male reproductive physiology. In humans, the about important male androgen is testosterone. Several accessory organs and ducts help the procedure of sperm maturation and transport the sperm and other seminal components to the penis, which delivers sperm to the female reproductive tract. In this department, we examine each of these different structures, and discuss the process of sperm product and transport.

Figure i. Click for a larger prototype. The structures of the male reproductive system include the testes, the epididymides, the penis, and the ducts and glands that produce and acquit semen. Sperm get out the scrotum through the ductus deferens, which is bundled in the spermatic cord. The seminal vesicles and prostate gland add fluids to the sperm to create semen.
Male REPRODUCTIVE SYSTEM - Testes – male gonads
- Seminiferous tubules – structures inside the testes that produce sperm – "sperm factories"
- Spermatogenesis – production of sperm cells by the seminiferous tubules; begins at puberty and is controlled by FSH and LH (besides known as interstitial jail cell-stimulating hormone – ICSH)
- Stages of sperm development:
- Spermatogonia – outermost cells of the seminiferous tubule that divides by mitosis to produce more cells
- Primary spermatocyte – inward spermatogonia that undergoes meiosis to produce sperm
- Secondary spermatocytes – 2 cells produced through the kickoff meiotic division
- Spermatids – 4 cells produced through the second meiotic division that mature into a sperm jail cell
- Accompaniment Ducts – ship sperm from the body
- Epididymis – caps the superior part of the testis and forms a temporary storage site for sperm to mature; takes x-fourteen days for sperm to mature in the epididymis
- Vas Deferens – carries sperm from the epididymus to the ejaculatory duct
- Ejaculatory duct – passes through the prostate gland to merge with the urethra; during ejaculation the thick walls of smoothen muscle create peristaltic waves that rapidly clasp the sperm forrad
- Urethra – carries both urine and sperm; sperm enters from ejaculatory duct, urine is coming from the bladder
- Accessory glands
- Seminal vesicle – produces lx% of seminal fluid; thick xanthous secretion that contains fructose, prostaglandins, and other substances to nourish and activate sperm; pH is slightly alkaline (basic)
- Prostate gland –doughnut-shaped gland that secretes a milky fluid that helps to actuate the swimming movements of sperm
- Bulbourethral gland – produces thick clear mucus that cleanses the urethra of acidic urine and lubricates the end of the penis in response to sexual stimulation
- Semen – mixture of sperm and accompaniment gland secretions
- External genitalia
- Scrotum – sac of pare that hangs exterior the intestinal cavity and encloses the testes; keeps testes virtually 3º lower than body temperature (necessary for good for you sperm)
- Penis – delivers sperm into female person reproductive tract
- The near important hormone of the testes is testosterone.
- Functions of testosterone:
- Stimulate reproductive organ evolution
- Promotes sexual practice drive
- Causes development of the secondary sexual activity characteristics – deepening of voice, increased hair growth, enlargement of skeletal muscles, thickening of bones
- Spermatogenesis – production of sperm cells by the seminiferous tubules; begins at puberty and is controlled by FSH and LH (besides known as interstitial jail cell-stimulating hormone – ICSH)
- Epididymis – caps the superior part of the testis and forms a temporary storage site for sperm to mature; takes x-fourteen days for sperm to mature in the epididymis
- Vas Deferens – carries sperm from the epididymus to the ejaculatory duct
- Ejaculatory duct – passes through the prostate gland to merge with the urethra; during ejaculation the thick walls of smoothen muscle create peristaltic waves that rapidly clasp the sperm forrad
- Urethra – carries both urine and sperm; sperm enters from ejaculatory duct, urine is coming from the bladder
Scrotum
The testes are located in a skin-covered, highly pigmented, muscular sack called the scrotum that extends from the trunk behind the penis. This location is important in sperm production, which occurs within the testes, and gain more efficiently when the testes are kept two to 4°C below core torso temperature.
The dartos musculus makes up the subcutaneous muscle layer of the scrotum. Information technology continues internally to make upwardly the scrotal septum, a wall that divides the scrotum into two compartments, each housing 1 testis. Descending from the internal oblique musculus of the intestinal wall are the two cremaster muscles, which cover each testis like a muscular net. Past contracting simultaneously, the dartos and cremaster muscles tin can drag the testes in cold weather (or water), moving the testes closer to the body and decreasing the surface area of the scrotum to retain heat. Alternatively, as the environmental temperature increases, the scrotum relaxes, moving the testes farther from the torso core and increasing scrotal expanse, which promotes heat loss. Externally, the scrotum has a raised medial thickening on the surface chosen the raphae.
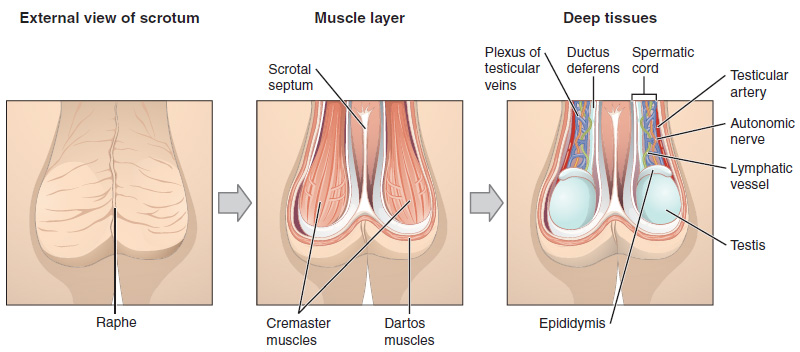
Figure two. This anterior view shows the structures of the scrotum and testes.
Testes
The testes (singular = testis) are the male person gonads—that is, the male reproductive organs. They produce both sperm and androgens, such as testosterone, and are agile throughout the reproductive lifespan of the male.

Figure 3. This sagittal view shows the seminiferous tubules, the site of sperm product. Formed sperm are transferred to the epididymis, where they mature. They leave the epididymis during an ejaculation via the ductus deferens.
Paired ovals, the testes are each approximately iv to five cm in length and are housed within the scrotum. They are surrounded past two distinct layers of protective connective tissue. The outer tunica vaginalis is a serous membrane that has both a parietal and a sparse visceral layer. Beneath the tunica vaginalis is the tunica albuginea, a tough, white, dense connective tissue layer covering the testis itself. Not merely does the tunica albuginea comprehend the outside of the testis, it also invaginates to form septa that divide the testis into 300 to 400 structures chosen lobules. Within the lobules, sperm develop in structures called seminiferous tubules. During the seventh month of the developmental menses of a male person fetus, each testis moves through the abdominal musculature to descend into the scrotal crenel. This is called the "descent of the testis." Cryptorchidism is the clinical term used when one or both of the testes fail to descend into the scrotum prior to nativity.
The tightly coiled seminiferous tubules form the bulk of each testis. They are composed of developing sperm cells surrounding a lumen, the hollow center of the tubule, where formed sperm are released into the duct system of the testis. Specifically, from the lumens of the seminiferous tubules, sperm motion into the straight tubules (or tubuli recti), and from there into a fine meshwork of tubules called the rete testes. Sperm leave the rete testes, and the testis itself, through the 15 to 20 efferent ductules that cross the tunica albuginea.
Inside the seminiferous tubules are 6 different jail cell types. These include supporting cells called sustentacular cells, too equally five types of developing sperm cells called germ cells. Germ cell development progresses from the basement membrane—at the perimeter of the tubule—toward the lumen. Permit's wait more closely at these prison cell types.
Sertoli Cells
Surrounding all stages of the developing sperm cells are elongate, branching Sertoli cells. Sertoli cells are a type of supporting cell called a sustentacular cell, or sustenocyte, that are typically found in epithelial tissue. Sertoli cells secrete signaling molecules that promote sperm product and can control whether germ cells alive or die. They extend physically around the germ cells from the peripheral basement membrane of the seminiferous tubules to the lumen. Tight junctions between these sustentacular cells create the blood–testis barrier, which keeps bloodborne substances from reaching the germ cells and, at the same fourth dimension, keeps surface antigens on developing germ cells from escaping into the bloodstream and prompting an autoimmune response.
Germ Cells
The least mature cells, the spermatogonia (singular = spermatogonium), line the basement membrane inside the tubule. Spermatogonia are the stalk cells of the testis, which means that they are even so able to differentiate into a multifariousness of different cell types throughout adulthood. Spermatogonia divide to produce principal and secondary spermatocytes, so spermatids, which finally produce formed sperm. The procedure that begins with spermatogonia and concludes with the production of sperm is chosen spermatogenesis.
Spermatogenesis
As only noted, spermatogenesis occurs in the seminiferous tubules that form the majority of each testis. The process begins at puberty, after which fourth dimension sperm are produced constantly throughout a man'southward life. 1 production bicycle, from spermatogonia through formed sperm, takes approximately 64 days. A new cycle starts approximately every 16 days, although this timing is non synchronous beyond the seminiferous tubules. Sperm counts—the total number of sperm a man produces—slowly turn down after age 35, and some studies suggest that smoking can lower sperm counts irrespective of historic period.
The process of spermatogenesis begins with mitosis of the diploid spermatogonia. Considering these cells are diploid (twon), they each have a complete copy of the begetter's genetic material, or 46 chromosomes. All the same, mature gametes are haploid (1n), containing 23 chromosomes—meaning that girl cells of spermatogonia must undergo a 2nd cellular division through the process of meiosis.
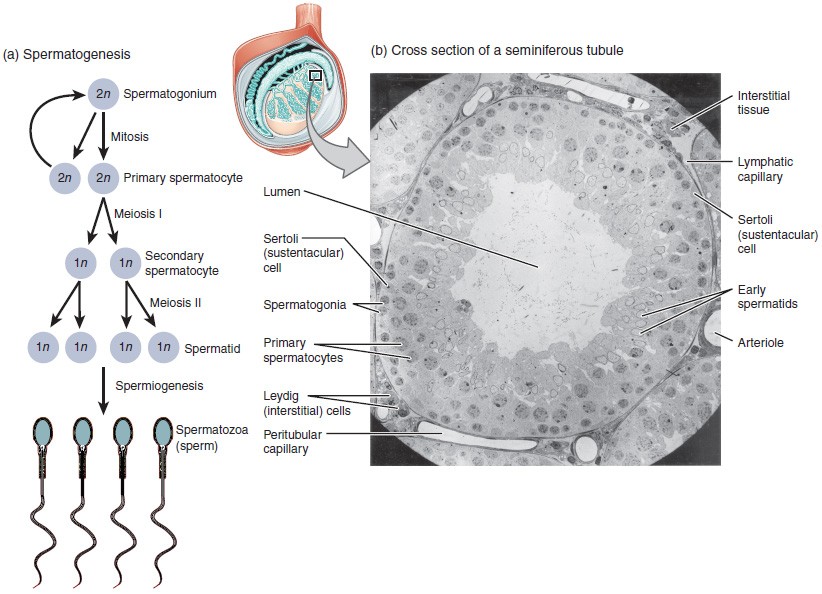
Figure 4. (a) Mitosis of a spermatogonial stem cell involves a single cell division that results in ii identical, diploid daughter cells (spermatogonia to main spermatocyte). Meiosis has two rounds of cell division: main spermatocyte to secondary spermatocyte, and then secondary spermatocyte to spermatid. This produces four haploid daughter cells (spermatids). (b) In this electron micrograph of a cross-department of a seminiferous tubule from a rat, the lumen is the light-shaded area in the center of the paradigm. The location of the primary spermatocytes is near the basement membrane, and the early spermatids are approaching the lumen (tissue source: rat). EM × 900. (Micrograph provided by the Regents of University of Michigan Medical Schoolhouse © 2012)
2 identical diploid cells event from spermatogonia mitosis. 1 of these cells remains a spermatogonium, and the other becomes a primary spermatocyte, the next stage in the process of spermatogenesis. As in mitosis, Dna is replicated in a master spermatocyte, and the jail cell undergoes cell sectionalization to produce two cells with identical chromosomes. Each of these is a secondary spermatocyte. At present a second circular of prison cell partitioning occurs in both of the secondary spermatocytes, separating the chromosome pairs. This 2d meiotic partition results in a full of 4 cells with only half of the number of chromosomes. Each of these new cells is a spermatid. Although haploid, early spermatids expect very like to cells in the earlier stages of spermatogenesis, with a circular shape, cardinal nucleus, and large amount of cytoplasm. A process called spermiogenesis transforms these early on spermatids, reducing the cytoplasm, and beginning the germination of the parts of a true sperm. The fifth stage of germ cell germination—spermatozoa, or formed sperm—is the end result of this procedure, which occurs in the portion of the tubule nearest the lumen. Eventually, the sperm are released into the lumen and are moved along a series of ducts in the testis toward a construction chosen the epididymis for the adjacent step of sperm maturation.
Structure of Formed Sperm
Sperm are smaller than virtually cells in the trunk; in fact, the book of a sperm cell is 85,000 times less than that of the female gamete. Approximately 100 to 300 meg sperm are produced each twenty-four hour period, whereas women typically ovulate only one oocyte per month as is true for most cells in the torso, the structure of sperm cells speaks to their function. Sperm have a distinctive head, mid-piece, and tail region. The head of the sperm contains the extremely compact haploid nucleus with very petty cytoplasm. These qualities contribute to the overall pocket-size size of the sperm (the head is only 5 μm long). A structure called the acrosome covers most of the caput of the sperm cell equally a "cap" that is filled with lysosomal enzymes important for preparing sperm to participate in fertilization. Tightly packed mitochondria fill up the mid-piece of the sperm. ATP produced by these mitochondria will ability the flagellum, which extends from the neck and the mid-piece through the tail of the sperm, enabling information technology to motility the entire sperm cell. The central strand of the flagellum, the axial filament, is formed from 1 centriole inside the maturing sperm cell during the final stages of spermatogenesis.

Figure 5. Sperm cells are divided into a head, containing Deoxyribonucleic acid; a mid-piece, containing mitochondria; and a tail, providing motility. The acrosome is oval and somewhat flattened.
Sperm Transport
To fertilize an egg, sperm must exist moved from the seminiferous tubules in the testes, through the epididymis, and—later during ejaculation—along the length of the penis and out into the female person reproductive tract.
Role of the Epididymis
From the lumen of the seminiferous tubules, the immotile sperm are surrounded by testicular fluid and moved to the epididymis (plural = epididymides), a coiled tube attached to the testis where newly formed sperm go on to mature. Though the epididymis does non take upwardly much room in its tightly coiled land, it would be approximately 6 m (20 feet) long if straightened. It takes an average of 12 days for sperm to move through the coils of the epididymis, with the shortest recorded transit time in humans being one day. Sperm enter the head of the epididymis and are moved along predominantly past the contraction of smooth muscles lining the epididymal tubes. As they are moved along the length of the epididymis, the sperm further mature and acquire the ability to move under their own power. In one case within the female person reproductive tract, they will use this ability to move independently toward the unfertilized egg. The more mature sperm are so stored in the tail of the epididymis (the final section) until ejaculation occurs.
Duct System
During ejaculation, sperm exit the tail of the epididymis and are pushed by smooth muscle wrinkle to the ductus deferens (too chosen the vas deferens). The ductus deferens is a thick, muscular tube that is bundled together within the scrotum with connective tissue, claret vessels, and nerves into a construction called the spermatic cord. Because the ductus deferens is physically attainable inside the scrotum, surgical sterilization to interrupt sperm commitment tin be performed by cut and sealing a minor section of the ductus (vas) deferens. This procedure is chosen a vasectomy, and information technology is an effective form of male birth command. Although it may be possible to contrary a vasectomy, clinicians consider the process permanent, and advise men to undergo it just if they are sure they no longer wish to father children.
Practice Question
Sentry this video to learn near a vasectomy. As described in this video, a vasectomy is a procedure in which a small section of the ductus (vas) deferens is removed from the scrotum. This interrupts the path taken by sperm through the ductus deferens. If sperm do non exit through the vas, either because the man has had a vasectomy or has not ejaculated, in what region of the testis practise they remain?
Prove Answer
Sperm remain in the epididymis until they degenerate.
From each epididymis, each ductus deferens extends superiorly into the abdominal cavity through the inguinal canal in the intestinal wall. From here, the ductus deferens continues posteriorly to the pelvic crenel, ending posterior to the bladder where it dilates in a region called the ampulla (meaning "flask").
Sperm make upward only five percent of the final book of semen, the thick, milky fluid that the male ejaculates. The majority of semen is produced by iii critical accessory glands of the male reproductive system: the seminal vesicles, the prostate, and the bulbourethral glands.
Seminal Vesicles
As sperm pass through the ampulla of the ductus deferens at ejaculation, they mix with fluid from the associated seminal vesicle. The paired seminal vesicles are glands that contribute approximately sixty pct of the semen volume. Seminal vesicle fluid contains large amounts of fructose, which is used past the sperm mitochondria to generate ATP to allow movement through the female person reproductive tract.
The fluid, at present containing both sperm and seminal vesicle secretions, side by side moves into the associated ejaculatory duct, a short construction formed from the ampulla of the ductus deferens and the duct of the seminal vesicle. The paired ejaculatory ducts transport the seminal fluid into the next structure, the prostate gland.
Prostate Gland
As shown in Figure 1, the centrally located prostate gland sits inductive to the rectum at the base of the bladder surrounding the prostatic urethra (the portion of the urethra that runs within the prostate). About the size of a walnut, the prostate is formed of both muscular and glandular tissues. It excretes an element of group i, milky fluid to the passing seminal fluid—at present called semen—that is critical to starting time coagulate and then decoagulate the semen following ejaculation. The temporary thickening of semen helps retain information technology within the female reproductive tract, providing fourth dimension for sperm to apply the fructose provided by seminal vesicle secretions. When the semen regains its fluid land, sperm tin then pass farther into the female reproductive tract.
The prostate normally doubles in size during puberty. At approximately age 25, it gradually begins to enlarge again. This enlargement does non usually crusade problems; however, abnormal growth of the prostate, or benign prostatic hyperplasia (BPH), can cause constriction of the urethra as information technology passes through the middle of the prostate gland, leading to a number of lower urinary tract symptoms, such as a frequent and intense urge to urinate, a weak stream, and a sensation that the bladder has not emptied completely. By age 60, approximately xl percent of men have some degree of BPH. By age 80, the number of affected individuals has jumped to equally many every bit lxxx per centum. Treatments for BPH attempt to salve the pressure level on the urethra so that urine can flow more than normally. Balmy to moderate symptoms are treated with medication, whereas severe enlargement of the prostate is treated by surgery in which a portion of the prostate tissue is removed.
Another mutual disorder involving the prostate is prostate cancer. According to the Centers for Disease Control and Prevention (CDC), prostate cancer is the second well-nigh common cancer in men. Nevertheless, some forms of prostate cancer grow very slowly and thus may non always crave treatment. Aggressive forms of prostate cancer, in contrast, involve metastasis to vulnerable organs like the lungs and brain. There is no link between BPH and prostate cancer, only the symptoms are similar. Prostate cancer is detected past a medical history, a blood exam, and a rectal examination that allows physicians to palpate the prostate and check for unusual masses. If a mass is detected, the cancer diagnosis is confirmed by biopsy of the cells.
Bulbourethral Glands
The final addition to semen is fabricated by 2 bulbourethral glands (or Cowper'south glands) that release a thick, salty fluid that lubricates the end of the urethra and the vagina, and helps to clean urine residues from the penile urethra. The fluid from these accessory glands is released after the male becomes sexually aroused, and shortly earlier the release of the semen. It is therefore sometimes called pre-ejaculate. Information technology is of import to note that, in addition to the lubricating proteins, information technology is possible for bulbourethral fluid to option upwards sperm already present in the urethra, and therefore information technology may be able to cause pregnancy.
Practise Question
Picket this video to explore the structures of the male reproductive system and the path of sperm, which starts in the testes and ends as the sperm leave the penis through the urethra. Where are sperm deposited after they get out the ejaculatory duct?
Evidence Answer
Sperm enter the prostate.
The Penis
The penis is the male organ of copulation (sexual intercourse). Information technology is flaccid for non-sexual actions, such every bit urination, and turgid and rod-like with sexual arousal. When erect, the stiffness of the organ allows it to penetrate into the vagina and deposit semen into the female reproductive tract.
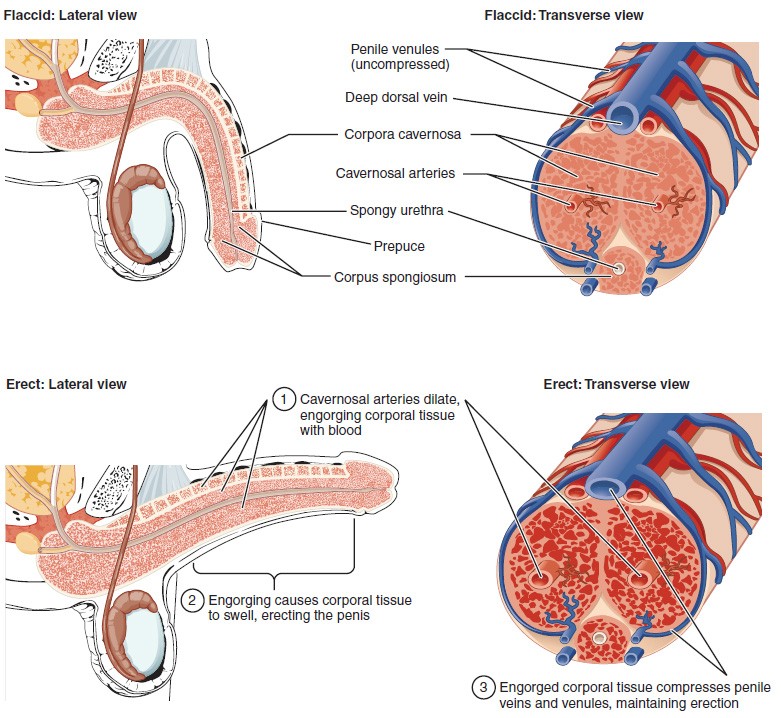
Effigy vi. Three columns of erectile tissue make up nearly of the volume of the penis.
The shaft of the penis surrounds the urethra. The shaft is composed of three column-like chambers of erectile tissue that span the length of the shaft. Each of the 2 larger lateral chambers is called a corpus cavernosum (plural = corpora cavernosa). Together, these brand up the bulk of the penis. The corpus spongiosum, which can be felt equally a raised ridge on the erect penis, is a smaller chamber that surrounds the spongy, or penile, urethra. The end of the penis, called the glans penis, has a high concentration of nervus endings, resulting in very sensitive skin that influences the likelihood of ejaculation. The skin from the shaft extends downwards over the glans and forms a collar called the prepuce (or foreskin). The foreskin also contains a dumbo concentration of nerve endings, and both lubricate and protect the sensitive pare of the glans penis. A surgical process called circumcision, often performed for religious or social reasons, removes the prepuce, typically within days of birth.
Both sexual arousal and REM sleep (during which dreaming occurs) tin can induce an erection. Penile erections are the result of vasocongestion, or engorgement of the tissues considering of more than arterial blood flowing into the penis than is leaving in the veins. During sexual arousal, nitric oxide (NO) is released from nerve endings near blood vessels within the corpora cavernosa and spongiosum. Release of NO activates a signaling pathway that results in relaxation of the smooth muscles that surround the penile arteries, causing them to dilate. This dilation increases the amount of blood that tin can enter the penis and induces the endothelial cells in the penile arterial walls to also secrete NO and perpetuate the vasodilation. The rapid increase in claret book fills the erectile chambers, and the increased pressure of the filled chambers compresses the thin-walled penile venules, preventing venous drainage of the penis. The result of this increased blood period to the penis and reduced blood return from the penis is erection. Depending on the flaccid dimensions of a penis, it can increase in size slightly or greatly during erection, with the average length of an erect penis measuring approximately 15 cm.
Disorders of the Male Reproductive System: Erectile dysfunction (ED)
Erectile dysfunction (ED) is a condition in which a man has difficulty either initiating or maintaining an erection. The combined prevalence of minimal, moderate, and complete ED is approximately 40 percent in men at age 40, and reaches almost 70 percent by 70 years of age. In addition to aging, ED is associated with diabetes, vascular disease, psychiatric disorders, prostate disorders, the utilize of some drugs such as certain antidepressants, and bug with the testes resulting in low testosterone concentrations. These physical and emotional weather condition tin lead to interruptions in the vasodilation pathway and consequence in an inability to achieve an erection.
Recall that the release of NO induces relaxation of the smooth muscles that surround the penile arteries, leading to the vasodilation necessary to achieve an erection. To contrary the process of vasodilation, an enzyme chosen phosphodiesterase (PDE) degrades a key component of the NO signaling pathway called cGMP. There are several different forms of this enzyme, and PDE type v is the type of PDE plant in the tissues of the penis. Scientists discovered that inhibiting PDE5 increases blood flow, and allows vasodilation of the penis to occur.
PDEs and the vasodilation signaling pathway are institute in the vasculature in other parts of the torso. In the 1990s, clinical trials of a PDE5 inhibitor chosen sildenafil were initiated to care for hypertension and angina pectoris (chest pain caused by poor blood flow through the heart). The trial showed that the drug was not effective at treating center conditions, but many men experienced erection and priapism (erection lasting longer than 4 hours). Because of this, a clinical trial was started to investigate the ability of sildenafil to promote erections in men suffering from ED. In 1998, the FDA canonical the drug, marketed as Viagra®. Since approval of the drug, sildenafil and similar PDE inhibitors at present generate over a billion dollars a year in sales, and are reported to exist effective in treating approximately seventy to 85 pct of cases of ED. Importantly, men with health problems—specially those with cardiac disease taking nitrates—should avoid Viagra or talk to their dr. to find out if they are a candidate for the employ of this drug, as deaths have been reported for at-risk users.
Testosterone
Testosterone, an androgen, is a steroid hormone produced by Leydig cells. The alternate term for Leydig cells, interstitial cells, reflects their location betwixt the seminiferous tubules in the testes. In male embryos, testosterone is secreted by Leydig cells past the 7th week of evolution, with peak concentrations reached in the 2nd trimester. This early release of testosterone results in the anatomical differentiation of the male person sexual organs. In childhood, testosterone concentrations are depression. They increase during puberty, activating characteristic physical changes and initiating spermatogenesis.
Functions of Testosterone
The continued presence of testosterone is necessary to keep the male reproductive system working properly, and Leydig cells produce approximately vi to vii mg of testosterone per day. Testicular steroidogenesis (the industry of androgens, including testosterone) results in testosterone concentrations that are 100 times higher in the testes than in the apportionment. Maintaining these normal concentrations of testosterone promotes spermatogenesis, whereas depression levels of testosterone can lead to infertility. In addition to intratesticular secretion, testosterone is also released into the systemic circulation and plays an of import office in muscle evolution, bone growth, the development of secondary sex characteristics, and maintaining libido (sex drive) in both males and females. In females, the ovaries secrete small amounts of testosterone, although most is converted to estradiol. A minor amount of testosterone is besides secreted by the adrenal glands in both sexes.
Control of Testosterone
The regulation of testosterone concentrations throughout the body is critical for male reproductive function. The intricate coaction betwixt the endocrine system and the reproductive arrangement is shown in Figure vii.

Figure 7. The hypothalamus and pituitary gland regulate the production of testosterone and the cells that assist in spermatogenesis. GnRH activates the anterior pituitary to produce LH and FSH, which in turn stimulate Leydig cells and Sertoli cells, respectively. The system is a negative feedback loop considering the stop products of the pathway, testosterone and inhibin, collaborate with the activity of GnRH to inhibit their own production.
The regulation of Leydig cell production of testosterone begins outside of the testes. The hypothalamus and the pituitary gland in the brain integrate external and internal signals to command testosterone synthesis and secretion. The regulation begins in the hypothalamus. Pulsatile release of a hormone called gonadotropin-releasing hormone (GnRH) from the hypothalamus stimulates the endocrine release of hormones from the pituitary gland. Binding of GnRH to its receptors on the anterior pituitary gland stimulates release of the two gonadotropins: luteinizing hormone (LH) and follicle-stimulating hormone (FSH). These 2 hormones are critical for reproductive role in both men and women. In men, FSH binds predominantly to the Sertoli cells within the seminiferous tubules to promote spermatogenesis. FSH also stimulates the Sertoli cells to produce hormones chosen inhibins, which office to inhibit FSH release from the pituitary, thus reducing testosterone secretion. These polypeptide hormones correlate directly with Sertoli jail cell role and sperm number; inhibin B tin can be used every bit a marking of spermatogenic activity. In men, LH binds to receptors on Leydig cells in the testes and upregulates the production of testosterone.
A negative feedback loop predominantly controls the synthesis and secretion of both FSH and LH. Low blood concentrations of testosterone stimulate the hypothalamic release of GnRH. GnRH then stimulates the anterior pituitary to secrete LH into the bloodstream. In the testis, LH binds to LH receptors on Leydig cells and stimulates the release of testosterone. When concentrations of testosterone in the blood reach a critical threshold, testosterone itself will bind to androgen receptors on both the hypothalamus and the anterior pituitary, inhibiting the synthesis and secretion of GnRH and LH, respectively. When the blood concentrations of testosterone over again refuse, testosterone no longer interacts with the receptors to the same caste and GnRH and LH are once once again secreted, stimulating more testosterone production. This same procedure occurs with FSH and inhibin to command spermatogenesis.
Aging and the Male person Reproductive Arrangement
Declines in Leydig cell activity tin occur in men beginning at 40 to 50 years of age. The resulting reduction in circulating testosterone concentrations can pb to symptoms of andropause, also known as male person menopause. While the reduction in sex steroids in men is akin to female menopause, in that location is no clear sign—such every bit a lack of a menstrual menses—to denote the initiation of andropause. Instead, men study feelings of fatigue, reduced muscle mass, depression, feet, irritability, loss of libido, and insomnia. A reduction in spermatogenesis resulting in lowered fertility is too reported, and sexual dysfunction can also be associated with andropausal symptoms.
Whereas some researchers believe that certain aspects of andropause are difficult to tease apart from aging in general, testosterone replacement is sometimes prescribed to convalesce some symptoms. Recent studies accept shown a do good from androgen replacement therapy on the new onset of low in elderly men; however, other studies caution confronting testosterone replacement for long-term treatment of andropause symptoms, showing that high doses tin sharply increase the risk of both heart disease and prostate cancer.
Affiliate Review
Gametes are the reproductive cells that combine to form offspring. Organs chosen gonads produce the gametes, along with the hormones that regulate man reproduction. The male person gametes are called sperm. Spermatogenesis, the product of sperm, occurs within the seminiferous tubules that make up most of the testis. The scrotum is the muscular sac that holds the testes exterior of the body crenel.
Spermatogenesis begins with mitotic sectionalization of spermatogonia (stalk cells) to produce primary spermatocytes that undergo the two divisions of meiosis to become secondary spermatocytes, then the haploid spermatids. During spermiogenesis, spermatids are transformed into spermatozoa (formed sperm). Upon release from the seminiferous tubules, sperm are moved to the epididymis where they continue to mature. During ejaculation, sperm exit the epididymis through the ductus deferens, a duct in the spermatic cord that leaves the scrotum. The ampulla of the ductus deferens meets the seminal vesicle, a gland that contributes fructose and proteins, at the ejaculatory duct. The fluid continues through the prostatic urethra, where secretions from the prostate are added to form semen. These secretions help the sperm to travel through the urethra and into the female reproductive tract. Secretions from the bulbourethral glands protect sperm and cleanse and lubricate the penile (spongy) urethra.
The penis is the male person organ of copulation. Columns of erectile tissue called the corpora cavernosa and corpus spongiosum fill up with blood when sexual arousal activates vasodilatation in the blood vessels of the penis. Testosterone regulates and maintains the sex activity organs and sexual practice drive, and induces the physical changes of puberty. Coaction between the testes and the endocrine organization precisely control the product of testosterone with a negative feedback loop.
Self Bank check
Reply the question(south) below to meet how well you sympathize the topics covered in the previous section.
Disquisitional Thinking Questions
- Briefly explain why mature gametes behave only i set of chromosomes.
- What special features are evident in sperm cells only not in somatic cells, and how do these specializations function?
- What do each of the three male accessory glands contribute to the semen?
- Describe how penile erection occurs.
- While anabolic steroids (synthetic testosterone) bulk up muscles, they can also touch on testosterone production in the testis. Using what you know almost negative feedback, describe what would happen to testosterone production in the testis if a male takes large amounts of constructed testosterone.
Glossary
blood–testis barrier: tight junctions between Sertoli cells that foreclose bloodborne pathogens from gaining admission to after stages of spermatogenesis and prevent the potential for an autoimmune reaction to haploid sperm
bulbourethral glands: (as well, Cowper's glands) glands that secrete a lubricating mucus that cleans and lubricates the urethra prior to and during ejaculation
corpus cavernosum: either of two columns of erectile tissue in the penis that fill with blood during an erection
corpus spongiosum: (plural = corpora cavernosa) column of erectile tissue in the penis that fills with blood during an erection and surrounds the penile urethra on the ventral portion of the penis
ductus deferens: (likewise, vas deferens) duct that transports sperm from the epididymis through the spermatic cord and into the ejaculatory duct; also referred every bit the vas deferens
ejaculatory duct: duct that connects the ampulla of the ductus deferens with the duct of the seminal vesicle at the prostatic urethra
epididymis: (plural = epididymides) coiled tubular structure in which sperm start to mature and are stored until ejaculation
gamete: haploid reproductive prison cell that contributes genetic material to form an offspring
glans penis: bulbous end of the penis that contains a big number of nerve endings
gonadotropin-releasing hormone (GnRH): hormone released by the hypothalamus that regulates the production of follicle-stimulating hormone and luteinizing hormone from the pituitary gland
gonads: reproductive organs (testes in men and ovaries in women) that produce gametes and reproductive hormones
inguinal canal: opening in intestinal wall that connects the testes to the intestinal crenel
Leydig cells: cells between the seminiferous tubules of the testes that produce testosterone; a type of interstitial cell
penis: male organ of copulation
prepuce: (also, foreskin) flap of skin that forms a collar effectually, and thus protects and lubricates, the glans penis; also referred every bit the foreskin
prostate gland: doughnut-shaped gland at the base of operations of the float surrounding the urethra and contributing fluid to semen during ejaculation
scrotum: external pouch of peel and muscle that houses the testes
semen: ejaculatory fluid composed of sperm and secretions from the seminal vesicles, prostate, and bulbourethral glands
seminal vesicle: gland that produces seminal fluid, which contributes to semen
seminiferous tubules: tube structures within the testes where spermatogenesis occurs
Sertoli cells: cells that support germ cells through the procedure of spermatogenesis; a type of sustentacular jail cell
sperm: (as well, spermatozoon) male gamete
spermatic cord: packet of nerves and blood vessels that supplies the testes; contains ductus deferens
spermatid: young sperm cells produced by meiosis Two of secondary spermatocytes
spermatocyte: cell that results from the sectionalisation of spermatogonium and undergoes meiosis I and meiosis II to form spermatids
spermatogenesis: germination of new sperm, occurs in the seminiferous tubules of the testes
spermatogonia: (singular = spermatogonium) diploid precursor cells that go sperm
spermiogenesis: transformation of spermatids to spermatozoa during spermatogenesis
testes: (singular = testis) male person gonads
Source: https://courses.lumenlearning.com/nemcc-ap/chapter/anatomy-and-physiology-of-the-male-reproductive-system/
0 Response to "what is the correct pathway for sperm from spermatogenesis to ejaculation"
Post a Comment